


What Gender-Affirming Care for Minors Actually Involves
The HHS report is lying

Last Thursday, I was in New York City for an LGBTQ health conference when Alex Sheldon, executive director of GLMA (an org for LGBTQ health providers), told me The Report was out. I knew which report they meant. I’d been expecting the “US version of the Cass Report” from the Department of Health and Human Services (HHS). My stomach dropped. I told Alex I want to both read every word so I can refute them all with scientific evidence and never, ever look at it.
The Cass Report is the common name for a report from the UK about gender-affirming care for minors. Despite its conclusions recommending what the standards of care already are (WPATH’s SOC8), despite the methods being shoddy, and despite the report being written by someone who doesn’t work in the field, the UK leveraged the report to severely restrict puberty blockers and hormones for trans/nonbinary youth. Then the anti-trans folks in the US pointed to the UK and said, “See, they banned care. We should too!”
The HHS report is supposedly about treating gender dysphoria in minors, but the recommendations are based on pseudoscience, selective reporting, and anti-trans bias. Though the report is anonymous, the authors have been uncovered. None of them have credentials in trans healthcare. Or even healthcare.1 It adds to the current anti-trans climate of misinformation and disinformation. It is propaganda.
So let’s get some things correct. I made the infographic below based on treatment guidelines from WPATH, the Endocrine Society, the American Academy of Pediatrics, the Dutch model, and UCSF.
What does gender-affirming care really mean?
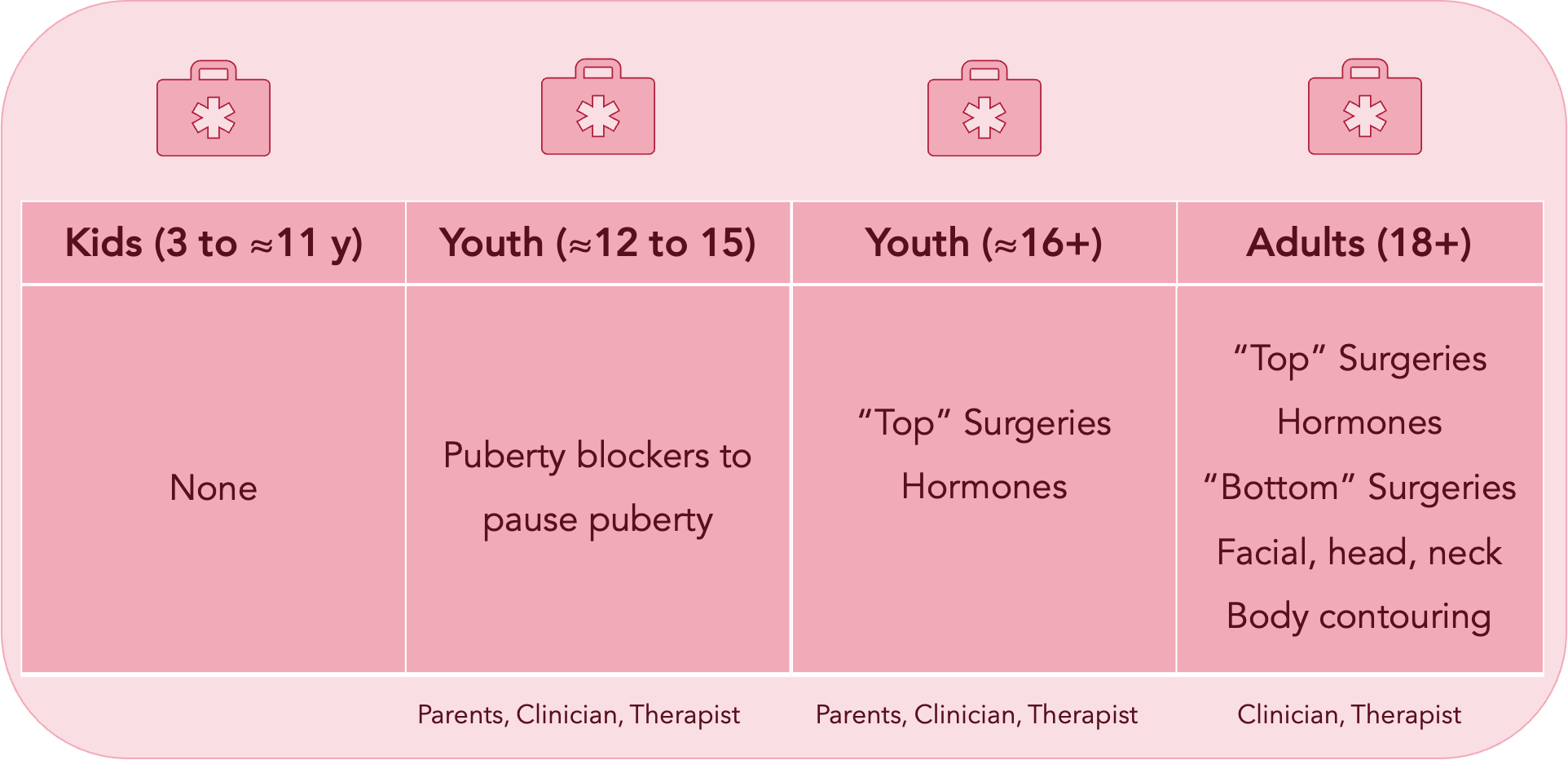
I’ve separated things by age group because age makes a huge difference in what is available.
Little Kids
The anti-trans movement uses a lot of scare tactics to rally people against gender-affirming care by spreading disinformation, especially around kids. (“chemical and surgical mutilation,” calling us gr00mers, etc.).
However, for pre-pubescent kids (approximately ages 3 to 11), there are no medical interventions. None.
All kids develop gender identity around ages 3 to 6 (I declared I’ll be a boy when I grow up when I was 3 years old). Cisgender kids have gender identities, too. That means kids as young as three may be telling and showing their parents things that indicate gender incongruence (a mismatch between sex assigned at birth and gender identity).
Gender-affirming care at this age means respecting the kid’s gender identity (through using their affirmed name and pronouns) while caring for the body that they have.
And peer-reviewed evidence shows that kids who have the support of their families in living as their affirmed gender have much better mental health than kids whose families do not support them. Affirmed trans kids have the same rates of mental health conditions as cis kids their age.
Family support is the primary intervention. (Family support involves making sure the schools and other institutions also affirm their kids.)
Pubescent Kids
Once kids start puberty, specifically Tanner Stage 2, they can be prescribed puberty blockers according to most guidelines.2 Kids reach Tanner Stage 2 around ages 9 to 11 for people assigned female at birth and age 11 for people assigned male at birth.
Puberty blockers (usually gonadotropin-releasing hormone agonists [GnRHa]) suppress hormones like testosterone and estrogen so that puberty doesn’t start. This prevents boys from growing breasts, curves, and having periods, and prevents girls from growing facial and body hair, growing taller and stronger, etc. Puberty is rough for everyone, but the distress from having the wrong puberty is damaging.
Once kids stop taking puberty blockers, their endogenous hormones kick in and puberty resumes as it would have otherwise. It does not cause infertility or other lasting changes. Trans kids who used puberty blockers first require lower doses of testosterone/estrogen and fewer surgeries.
Multiple studies show that withholding puberty blockers causes irreversible damage (e.g., breasts that then have to be removed) and mental harm.3
Note that to obtain puberty blockers, kids need involvement and permission from parents, clinicians, therapists, and insurance companies.
Older Teenagers
Depending on the kid (with their parents, clinicians, and therapists), teen minors may access hormones. Guidelines usually say this is for kids aged 16 and older, but others recommend considering it on a case-by-case basis. An analysis of an extensive insurance database with 5 million kids aged 8-17 found a tiny number of kids who accessed hormones as young as 12, but none younger than that. Starting hormones peaked at age 17 in the database.4
Some older teens 16 and older, especially transmasculine people and nonbinary people assigned female at birth, may also get chest surgery, or what we call “top surgery.” Fewer than 300 trans youth per year get top surgery before age 18.5 Again, permission is required from parents, clinicians, and therapists.
Note that cisgender girls make up 87% of all breast reduction surgeries in the US. And they get those surgeries on average two years younger than trans kids do.6
Very rarely, older teens, 17-year-olds, may get bottom (genital) surgery; the numbers are extremely low. One analysis looked at data from 2019 to 2021 and found 56 minors who had any genital surgery.7
Adults
Once they are 18, trans and nonbinary people are allowed to access any of the possible hormonal and surgical interventions, with clinician and therapist approval. And insurance. And the financial means. And support for post-surgical care. And the ability to take time off work.
Gender-affirming medical care is lifesaving, essential healthcare.
The report's authors appear to be Alex Byrne (an MIT philosophy professor), John Koenig (degrees in English and Business), and Blake Sanchez (a BS in neuroscience). The names were found in the report metadata. Early analysis shows AI-generated content, and considering how quickly the report was launched, that seems likely. In my experience consulting for a federal agency, reports take well over a year to conceive, write, review, and launch.
The Dutch approach requires age 12 rather than a puberty stage.
Hughes, L. D., Charlton, B. M., Berzansky, I., & Corman, J. D. (2025). Gender-Affirming Medications Among Transgender Adolescents in the US, 2018-2022. JAMA Pediatr.
https://www.reuters.com/investigates/special-report/usa-transyouth-data/
Hassan, B., Zeitouni, F., Ascha, M., Sanders, R., Berger, Z., Fields, E., & Liang, F. (2024). Breast Surgery in Adolescents: Cisgender Breast Reduction Versus Transgender and Nonbinary Chest Masculinization. Ann Plast Surg, 93(2), 194-199
https://www.reuters.com/investigates/special-report/usa-transyouth-data/
Great information, thank you for sharing it.